Articles
- Page Path
- HOME > Perspect Integr Med > Volume 3(1); 2024 > Article
-
Original Article
Effects of Pulsed Electromagnetic Field Therapy and Photontherapy in Cervicobrachialgia: A Randomized Controlled Trial -
Bianca dos Santos Bobadilha1
 , Talita Bonato de Almeida2, Maria Imaculada de Lima Montebello3, Maria da Luz Rosário de Sousa4,*
, Talita Bonato de Almeida2, Maria Imaculada de Lima Montebello3, Maria da Luz Rosário de Sousa4,* -
Perspectives on Integrative Medicine 2024;3(1):37-44.
DOI: https://doi.org/10.56986/pim.2024.02.005
Published online: February 22, 2024
1Department of Health Sciences and Pediatric Dentistry, Piracicaba Dental School, State University of Campinas (Unicamp), São Paulo, Brazil
2Anhembi Morumbi University, Piracicaba / São Paulo, Brazil
3Postgraduate Program in Movement Sciences and Administration, Methodist University of Piracicaba, Piracicaba / São Paulo, Brazil
4Department of Health Sciences and Pediatric Dentistry, Piracicaba Dental School, State University of Campinas (Unicamp), Piracicaba / São Paulo, Brazil
- *Corresponding author: Maria da Luz Rosário de Sousa, Department of Health Sciences and Pediatric Dentistry, Piracicaba Dental School, State University of Campinas (Unicamp) Av. Limeira, 901, Areião, 13414-018, Piracicaba / São Paulo, Brazil, Email: luzsousa@fop.unicamp.br
©2024 Jaseng Medical Foundation
This is an open access article under the CC BY-NC license (http://creativecommons.org/licenses/by-nc/4.0/).
- 531 Views
- 10 Download
Abstract
-
Background
- Cervicobrachialgia is a painful condition commonly treated with medication and physiotherapy. The aim was to evaluate pain following electromagnetic and photontherapy, and examine patient energy profiles.
-
Methods
- There were 48 patients experiencing pain [Visual Analogue Scale (VAS) score ≥ 4] who were not receiving medication and physiotherapy and were randomized into Test Group (GT); electromagnetism using a Kenkobio device (intensity = 0.055 mT/frequency = 60 Hz) and photon therapy; a photon therapy blanket, and Placebo Group (GP); the Kenkobio device was turned off and the blanket was not used. Pain was assessed using the VAS, before, immediately after treatment, and the following day. Algometry was also carried out before and after the treatment to understand the pain threshold at bilateral acupoints GB20 and GB21. The energy profile was assessed using Ryodoraku measurements before and after the session.
-
Results
- The GT achieved a greater reduction in pain the following day than GP. Both groups were equal for left GB20 and right GB21 points considering algometry and, after the intervention, a reduction in pain in the GT was noticed only in the left GB20 (CI [95%]: 0.09–0.99, p = 0.019). The average energy level was low and dropped further following treatment. Furthermore, energy from the Large Intestine Meridian tended towards balance in the GT compared with the GP [CI (95%): 0.58–15.75, p = 0.035]. No adverse effects were reported.
-
Conclusion
- The combined use of electromagnetic and photontherapy were effective in reducing pain in patients and promoted energy rebalancing.
- Neck pain (cervicobrachialgia) is characterized by pain in the spine in the cervical region which radiates down the arm due to compression or pinching of the nerve roots in this region. Neck pain has an incidence of 10.4–21.3% per year in the US [1], and is the 8th cause of disability worldwide for women, and the 12th for men [2].
- For the treatment of neck pain, conventional therapies such as cervical stretching and strengthening exercises [3], and the use of non-steroidal anti-inflammatory drugs can be used to relieve pain in the spine [4]. In addition, local electrical and electromagnetic stimuli can be used [5], which promote the release of neurotransmitters in the central nervous system, as well as other substances responsible for analgesia, restoration of organic functions, and immune modulation [6].
- There are some literature reviews on the use of electro-magnetic fields in healthcare, but most of the reviewed studies were conducted in vitro. The findings suggest that pulsed electromagnetic field promotes the proliferation of osteoblasts when its frequency is 7.5–15 Hz or 50–75 Hz and the intensity is 0.40–1.55 mT or 3.8–4 mT, and when associated with an electromagnetic field sinusoidal and static magnetic field, osteoblast differentiation and maturation are promoted [7]. A review of human and animal studies demonstrated that chronic exposure of more than 22 days to an electromagnetic field of approximately 30 μT reduced levels of the hormone melatonin in rats and humans [8].
- Pulsed Electromagnetic Field Therapy (TCEP) is an example of the use of electromagnetic stimuli in healthcare and is authorized for use and regulated by the United States Food and Drug Administration for the treatment of fracture injuries [9]. The review demonstrated an improvement in osteoblastogenesis and inhibition of osteoclastogenesis for promoting fracture healing caused by postmenopausal osteoporosis using a pulsed electromagnetic field that contributed to an increase in bone mass and strength [9]. A study to examine TCEP therapy for women with fibromyalgia reported the therapy may improve function, fatigue, and pain [10]. A cohort demonstrated that the use of TCEP is safe in patients with chronic neck pain but did not cause changes in the pain threshold of these patients [11].
- Photontherapy is another example of electromagnetic application in healthcare, consisting of the use of long infrared rays between 4 and 14 μm, which cause beneficial effects in oncology similar to those of solar radiation [12]. Photontherapy requires heat for activation, with the emission of infrared rays increasing with temperature [12]. For this purpose, devices that generate heat in a controlled manner can be used. Positive effects of photontherapy has been reported to reduce the effects of stress, improve blood oxygenation, reduce inflammation, and improve muscle function [12]. Stimulation with sufficient intensity and duration induces a current through the target cell membranes, activating nerve cells or muscles to propagate action potentials [11].
- A study conducted on patients with shoulder pain reported that the use of photontherapy for an average of 4 weeks reduced pain by 75% using the self-reported visual analogue scale (VAS), where the numerical quantification scale 0 (no pain) to 10 (worst possible pain) is employed [13].
- Few studies have combined 2 or more electromagnetic therapies and used instruments to compare and verify pain after their use. Therefore, the objective of this study was to evaluate whether electromagnetic field therapy and photontherapy could reduce pain related to cervicobrachialgia and to evaluate the energy pattern of these patients before and after using them.
Introduction
- This study was approved by the Research Ethics Committee of the Piracicaba Dental School (CAAE: 34463820.0.0000.5418) and the Brazilian Clinical Trials Registry - REBEC (no.: RBR-96bkkj7).
- 1. Location
- Volunteers were recruited from the Piracicaba Dental School and the Primary Care Reference Center (CRAB) in the Cecap neighborhood in the municipality of Piracicaba / São Paulo.
- 2. Inclusion and exclusion criteria
- To participate in the clinical study, male and female volunteers must be aged 18 or over and under 65 years, and report cervicobrachial pain with an intensity ≥ 4 on the VAS. In the present study, the pain parameter related to cervicobrachialgia was obtained through the patient’s self-report, including pain in the cervical region of any origin, which may radiate to the neck and arms, without medical or physiotherapeutic diagnostic tests being used as an inclusion criterion. Excluded from the study were pregnant women, those with cardiac pacemakers or other electronic implants, post-traumatic neck pain, patients with visual and auditory disorders, sleep, cognition, and emotional disorders, and individuals who were using analgesics, muscle relaxants, and anti-inflammatories in the last 12 hours. Volunteers were invited to participate in the research and signed the Free and Informed Consent Form.
- 3. Description of the groups and therapeutic intervention
- After performing the initial VAS assessment, algometry assessment, and Ryodoraku measurements, volunteers were randomized into 2 study groups: the Test Group (GT) and the Placebo Group (GP). Participants in the GT underwent a single TCEP session with the Kenkobio electromagnetic device (Kenko Patto® brand), applied at an intensity of 0.055 mT and a frequency of 60 Hz.
- In this study, we used a Kenkobio device with a photon blanket at acupuncture points. The Kenkobio device emits heat during the operation time, reaching ideal functioning between 37 and 40°C, which is the temperature at which the electromagnetic field is stable, safe, and suitable for therapeutic use. The safety of the device is guaranteed by an automatic transducer, which causes the device to switch off at temperatures above 60°C. The Kenkobio device was wrapped in a photon blanket called a PhotonBag (Kenko Patto® brand) for the application of photon therapy, which comprises monofilament thermoplastic fibers of an elastic polyurethane polymer, approximately 8 μ in diameter, among which is the powder of incorporated colloidal platinum of size 40 A, particulate titanium with 0.24 μ (maximum), and particulate aluminum with 0.34 μ (maximum). The blanket is capable of selectively emitting an infrared electromagnetic wave between 4 and 14 μm, normally radiating between 9 and 10 μ at around 37°C (normal human temperature). The blanket was activated by the heat generated by the Kenkobio device, reaching ideal radiation conditions in the first minute of use. The blanket also acts as a thermal insulator, preventing the heat generated by the Kenkobio device from causing discomfort or burns.
- The Kenkobio device was applied to certain areas of the volunteer’s body, following the treatment protocol described by Perez [14] based on bioenergetics (Table 1). The device was kept in the areas and duration indicated in the protocol, one by one, and the areas were changed by the researcher. In the last stage of the protocol, the device was positioned on the most painful area for the patient (this area varied for each patient). The session lasted approximately 30 minutes. After the session, the analysis instruments were applied again.
- The GP volunteers experienced the same GT protocol, that is, the pain parameters and the Ryodoraku measurements were collected, the patient remained accommodated for 30 minutes and the device was positioned in the same areas indicated in the GT. However, the Kenkobio device was not connected to the socket, and therefore did not emit heat, and the blanket was not used around the device.
- After the research had been completed volunteers could access treatment with acupuncture in the Piracicaba Dental School and in the Primary Care Reference Center.
- 4. Outcomes
- After completing the protocol, volunteers from both groups had carried out the VAS assessments, performed algometry assessments at predefined points, and had their energy checked using the Ryodoraku measurement method. The VAS was used to record patient pain experienced in the cervical region (self-reported pain scale) using the following question, “On a scale of 0 to 10, with 0 being no pain and 10 being the worst possible pain, what grade would you give to your pain?” The VAS score was collected before the start of the protocol (VASi), immediately after removing the device (VASf), and the day after the session had been conducted via phone call or WhatsApp (VASl).
- To measure pain sensitivity, algometry assessments were performed using an algometer (Kenko Patto® brand, model DDK) which indicates the pressure in kgf/cm2 (through a digital display) at which the pain threshold is experienced by the patient. Contact of the algometer with the patient’s skin was made through a stimulation probe with a diameter of 1.0 cm2. This measurement was performed bilaterally at points GB20 (Fengchi), located in the bone recess between the external occipital tuberosity and the mastoid process, and GB21 (Jianjing), located on the lateral side of the neck between the vertebral column and the acromion of the shoulder [11].
- The Ryodoraku method was used to measure an individual’s circulating energy, and was performed using 12 specific bilateral acupuncture points [15] which have lower electrical resistance and greater electrical current intensity. For this purpose, the Ryodoraku device (RDK/NKL - Produtos Eletrônicos Ltda. Brusque / SC, Brazil / lot 00218) was used. The points used refer to the respective meridians, with 12 located on the wrists of the right and left hands (LU9, PC7, HT7, SI5, TE4 and LI5), and 12 located on the right and left feet (SP3, LR3, KI3, BL64, GB40, ST42) [16,17]. The Ryodoraku device consists of a portable unit, with a USB port for connection to a computer, and has 2 electrodes, one of the electrodes being a return rod, which the patient holds with the hand, and the other, a probe that allows the placement of a cotton tip (swab) that was moistened in water and touched to the patient’s skin at specific points. The values are expressed as μA in a graph, representing the right and left sides of each meridian. According to Ryodoraku’s theory, individuals with well-balanced energy would form a line across the graph, ideally at 50 μA, with a normal range between 40 and 60 μA. Values above or below this range indicate some energy change, which may be an excess or a deficiency [14].
- 5. Statistical analysis
- To analyze the results of the VAS assessments, algometry assessments and Ryodoraku measurement parameters comparing before and after the session, the Student test was used for intragroup analysis and the analysis of variance (ANOVA) was used for Repeated Measures for comparisons between groups, followed by the post hoc Bonferroni correction.
- The analysis of the VAS scores were carried out for the initial, final, and late assessments, and for algometry assessments, and the analysis of before and after the session at acupoints GB20 and GB21 was performed.
- For the Ryodoraku measurement analysis, the general energy average and the averages before and after carrying out the protocol were evaluated for all meridians to understand the energy patterns already carried by the patients before the session and the possible changes caused by the therapy. The difference in values between the left and right sides of each meridian, called laterality, was also checked before and after the session, in order to check whether the therapy changed this value. The greater the laterality value, the greater the imbalance between the right left sides of that meridian.
- The significance level adopted for the tests was 5%. SPSS Version 21 was used to perform statistical analysis of the data.
- 6. Sample calculation
- The sample calculation was carried out in the G*Power software (Version 3.1.9.4), using the within factors comparison method (repeated measures), based on a pilot study using the assessment values for algometry at the GB21 acupoint. Considering a Type 1 error of 5%, a sample power of 95%, and an average effect f = 0.37, 18 individuals would be needed in each group to detect potential differences. In order to reduce the effects of possible losses, a margin of 20% was added to the sample calculation, and so the final number of individuals per group was 24.
- 7. Randomization
- Volunteers were randomized into study groups using premade opaque paper envelopes, which identified the target study group, and each participant chose their envelope.
- 8. Blinding
- Only the volunteers were blinded to the groups and interventions, as the therapies were applied by the researcher.
Materials and Methods
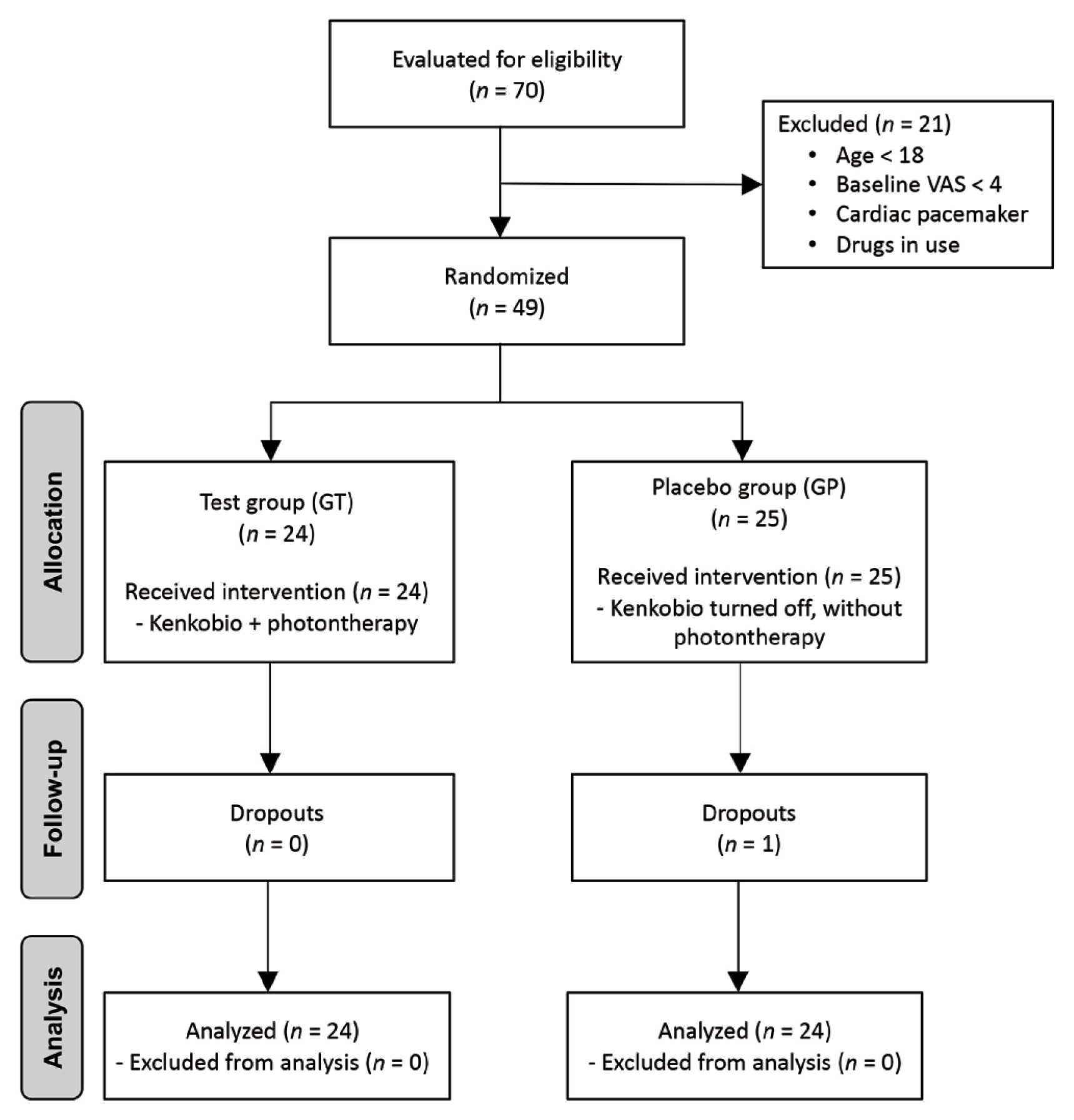
- A total of 48 volunteers participated in this study, which was randomized similarly among the groups (Fig. 1). The treatment protocol for the Kenkobio device used with a photon blanket at specific acupuncture points are shown in Table 1. The study began with groups of equal characteristics (p > 0.05), except for algometry assessment values for the right GB20 point [confidence interval (CI) (95%):0,16–1.13, p = 0.01] and left GB21 point [CI (95%): 0.30–2.01, p = 0.009; Table 2]. The means and SDs of the initial, final, and late VAS scores are shown in Table 3. The VAS score in the GT decreased immediately after the session, and decreased on the following day (VASl). The VAS scores in the GP also decreased after the session; however, on the following day, it increased again, indicating that the GT had significantly less pain than the GP the day following treatment [CI (95%):−3.67- -0.33, p = 0.020; Table 3]. The algometry measurements (Table 4) demonstrated that at the beginning of the study, both groups were not significantly different for the left GB20 and right GB21 points. After the intervention, when analyzing these points, a reduction in pain in the GT was noticed only in the left GB20 [CI (95%): 0.09–0.99, p = 0.019]. The analysis of the general energy and of each meridian verified by Ryodoraku measurements is shown in Table 5. It was observed that the general energy after the intervention decreased in both groups, and that in the GT, there was a statistically significant reduction in all meridians, except the Kidney meridian [CI (95%): −0.20–8.91, p = 0.061]. In GP, it was observed that 6 of the 12 meridians analyzed significantly had a decreased amount of energy after therapy (Table 5).
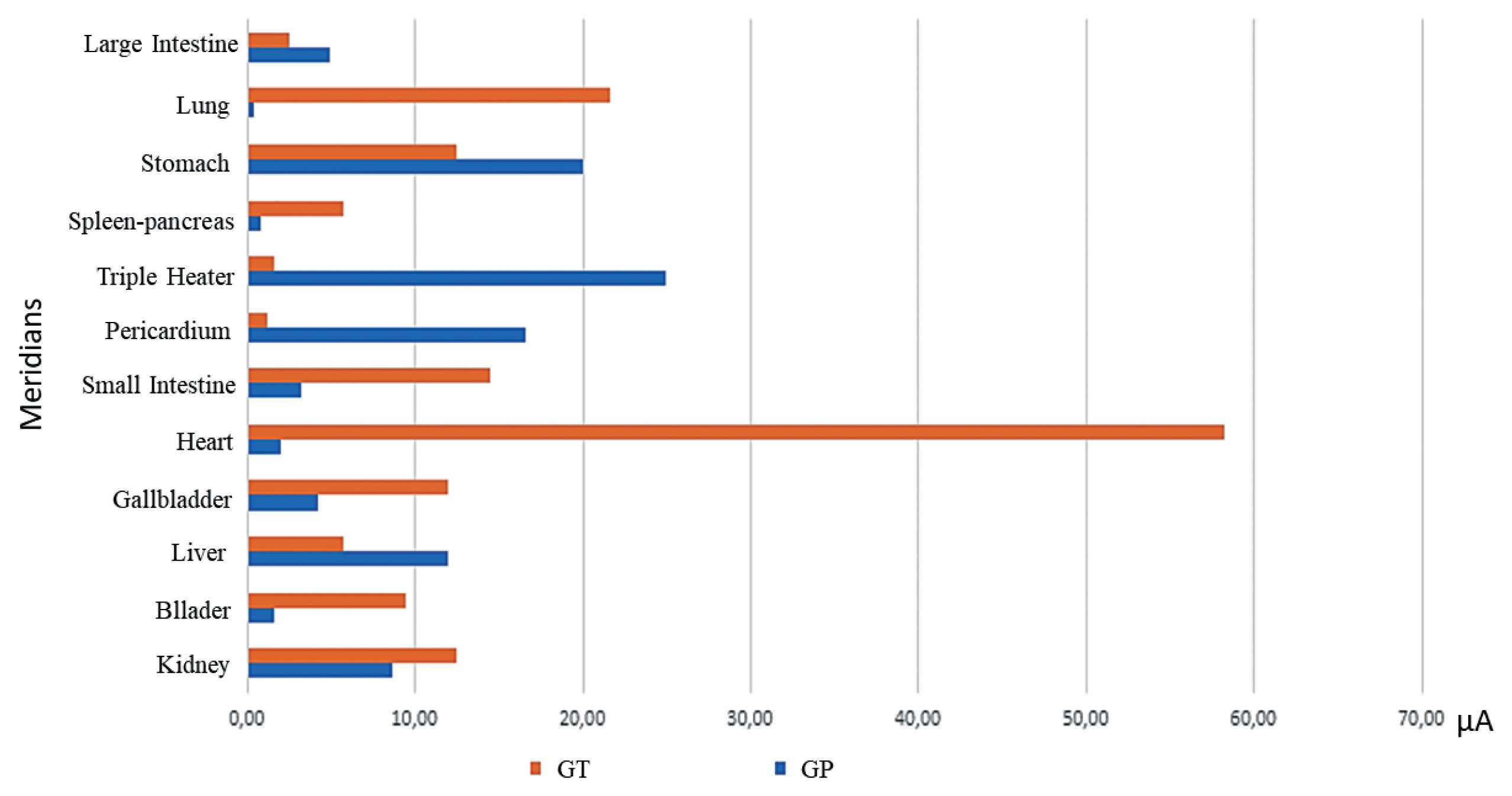
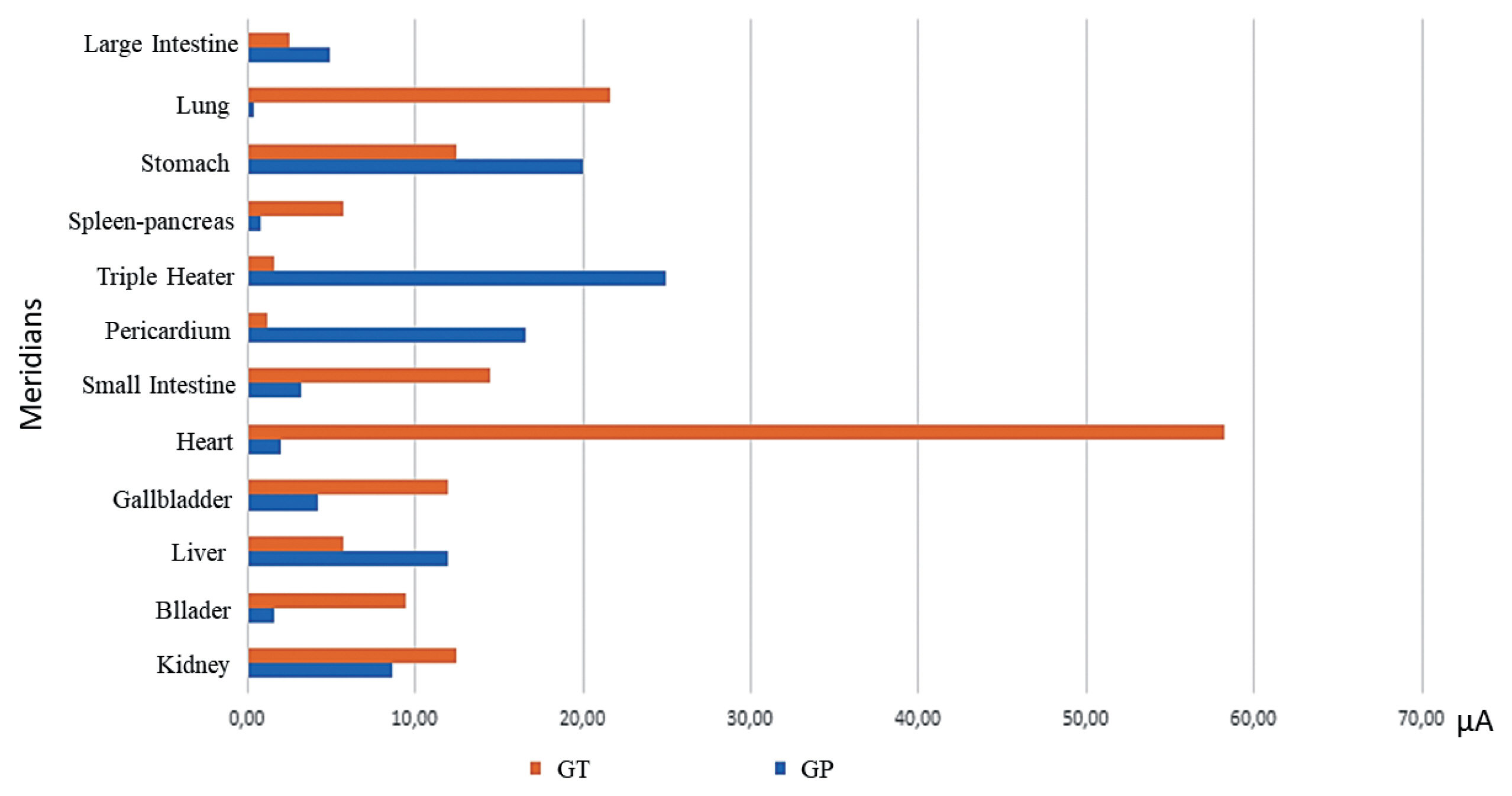
- The analysis of the energy imbalance of each meridian after therapy in both groups is shown in (Fig. 2). Visually, it was verified that in the GT, there was a greater energy imbalance between the right and left sides in the heart and lung meridians. Furthermore, where there was greater balance in GT was in the Triple Energizer and Pericardium compared with the placebo, as shown in (Fig. 2).
Results
- Electromagnetic and photontherapy combined therapies in this study were effective in reducing pain and promoted energy rebalancing in patients with cervicobrachialgia. These results are promising because the combined use of Kenkobio and photontherapy showed a reduction in neck pain which remained beneficial until the next day.
- A systematic review showed the beneficial effect of TCEP on pain, stiffness, and physical function in patients with osteoarthritis; however, it points to the need for more studies to confirm the effects of the therapy [18]. In the study by Karakas et al [10], TCEP was used to treat patients with chronic neck pain, and they reported the reduction in pain was 62.50% using the VAS, whereas in our study, the reduction in pain due to cervicobrachialgia from before treatment compared with the following day in the GT was 59.04%, similar to the data on pain reduction in patients with musculoskeletal pain.
- The intensity and frequency of electromagnetic fields used for therapeutic purposes remain heterogeneous, without consensus or standardization for their use. However, studies have reported therapeutic properties while using an intensity from 4.35 μT to 8 T and a frequency between 0 and 54 GHz [19,20]. These parameters for intensity and frequency were used in the present study.
- In a systematic review of the influence of the stimulatory frequency involved in the analgesic effects induced by electroacupuncture in tension neck pain, the combined use of acupuncture, auriculotherapy, Yamamoto new scalp acupuncture, koryoacupuncture, or chiroacupuncture, and electroacupuncture in patients with neck pain showed statistically significant positive results in reducing self-reported pain by patients [21]. The study that used a frequency of 100 Hz showed a reduction in self-reported pain of 41.92% (p = 0.013), the frequency used in our study was 60 Hz and showed a reduction in self-reported pain of 59.04%.
- The algometer instrument was important for the objective assessment of pain because when pressing the GB20 point, which is sensitive in patients with cervicobrachialgia, there was proposed to be a greater resistance to withstand the pain after the intervention, which may be a good way to evaluate the results of these therapies.
- Manafnezhad et al [22] used an algometry assessment to evaluate patients with non-specific neck pain using trigger point needling as therapy, however, no significant difference in pain intensity between the test and placebo groups was observed.
- In the present study, TCEP (as measured by Ryodoraku values), caused a decrease in the average general energy of individuals after its application, an effect previously reported with the use of acupuncture [23]. All meridians were energy deficient (< 40 μA) before the therapy was carried out. According to traditional Chinese medicine (TCM), when the Pericardium meridian has insufficient energy, it is common for the patient to experience stiffness and pain in the head and neck [14,24], as observed in the present study. The Kidney was the meridian that suffered the least changes due to the use of therapy, showing more stability in both the GT [CI (95%): −0.20–8.91, p = 0.061] and the GP [CI (95%): −0.70–8.41, p = 0.095], which can be explained in TCM terms that the kidney stores ancestor energy of the individual, which tends not to change due to external causes, and the Jing (essence) is stored [24]. There was a visual tendency towards greater energy rebalancing in the GT group (difference close to zero after therapy) than in the GP group; however, there was no statistical difference observed between the groups for any meridian. In future studies evaluating energy balance in the meridians after using therapies, it will be possible to use the data from the present work to provide an adequate and targeted sample calculation to achieve the design effect of the study.
- The Large Intestine, Liver, Small Intestine, Pericardium and Triple Energizer meridians were the meridians that most reduced the imbalance in GT. In the present study, the Heart and Pericardium in the GP were the meridians that tended towards balance. These meridians, being related to the reduction of agitated emotional states, may have balanced without the therapy being involved. The placebo effect involves a complex neurobiological reaction that includes everything from an increase in neurotransmitters such as endorphins and dopamine to greater activity in some regions of the brain linked to mood and emotional reactions [25].
- The Fire element, which is related to emotions by TCM [24], showed energy balance in the Yang Triple Energizer and Pericardium, but this did not occur in the Yin meridians, as the study was carried out in a single session for each individual.
- The concomitant use of Kenkobio and the photonic blanket did not allow us to discern whether the beneficial effect observed was due to one of the therapies or their combined use, which is a limitation of this study. Furthermore, the fact that the study was started with different pain thresholds between the groups according to algometry measurements at the left GB21 and right GB20 points can be considered as a limitation, so it is recommended that future studies initially screen patients for this parameter.
- More studies need to be conducted in this new field of energy measurement so that this therapy advances and its treatment is more individualized.
Discussion
- Combined electromagnetic therapy and photontherapy were effective in reducing pain in patients with cervicobrachialgia and promoted some energy rebalancing. However, more studies are needed to expand the understanding of this energy balance.
Conclusion
-
Authors Contributions
Conceptualization: BSB and MLRS. Methodology: BSB and MLRS. Formal investigation: BSB and MLRS. Data analysis: MILM. Writing original draft: BSB and TBA. Writing - review and editing: TBA and MLRS.
-
Conflicts of Interest
There are no conflicts of interest associated with this publication.
-
Funding
The study was financed by the São Paulo State Research Support Foundation - “Fundação de Amparo à Pesquisa do Estado de São Paulo” (FAPESP) - Process Number: 2020/06875-2.
-
Ethical Statement
This study was approved by the Research Ethics Committee of the Piracicaba Dental School (CAAE: 34463820.0.0000.5418) and the Brazilian Clinical Trials Registry - REBEC (no.: RBR-96bkkj7).
Article information
Data Availability

| Variables | Test group (n = 24) | Placebo group (n = 24) | CI (95%), p* |
|---|---|---|---|
| Age (y) | 41.46 ± 13.08 | 33.71 ± 14.2 | −0.19–15.69, 0.055 |
|
|
|||
| Sex, n (%) | 0.683 | ||
| Female | 21 (87.5) | 20 (83.3) | |
| Male | 3 (12.5) | 4 (16.7) | |
|
|
|||
| Initial† VAS score | 6.96 ± 1.75 | 6.21 ± 0.36 | −0.27–1.77, 0.145 |
|
|
|||
| Initial† algometry measurement (kgf/cm2) | |||
| GB20 right | 2.56 ± 0.87 | 1.92 ± 0.79 | 0,16–1.13, 0.010 |
| GB20 left | 2.53 ± 0.69 | 2.66 ± 0.85 | −0.58–0.33, 0.574 |
| GB21 right | 4.07 ± 1.43 | 3.60 ± 1.43 | −0.36–1.30, 0.261 |
| GB21 left | 4.25 ± 1.59 | 3.09 ± 1.34 | 0.30–2.01, 0.009 |
| General energy (mA) | 19.63 ± 9.86 | 18.83 ± 12.18 | −5.65–7.23, 0.806 |
| Test group (average VAS scores ± SD) | Placebo group (average VAS scores ± SD) | CI (95%), p | |
|---|---|---|---|
| Initial* | 6.96 ± 1.75 | 6.21 ± 1.75 | −0.27–1.77, 0.145 |
| Final† | 4.25 ± 2.54 | 5.21 ± 2.54 | −2.43–0.52, 0.197 |
| Late‡ | 3.50 ± 2.87 | 5.50 ± 2.87 | −3.67- -0.33, 0.020 |
| Algometry measurement (kgf/cm2) | Before intervention | After intervention | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| Test group | Placebo group | CI (95%), p* | Test group | Placebo group | CI (95%), p* | |
| GB20 right | 2,564 | 1,918 | 0.16–1.13, 0.010 | 2,636 | 1,898 | 0.18–1.30, 0.011 |
|
|
||||||
| GB20 left | 2,529 | 2,656 | −0.58–0.33, 0.574 | 2,491 | 1,948 | 0.09–0.99, 0.019 |
|
|
||||||
| GB21 right | 4,075 | 3,604 | −0.36–1.30, 0.261 | 4,214 | 3,418 | −0.21–1.80, 0.117 |
|
|
||||||
| GB21 left | 4,246 | 3,091 | 0.30–2.01, 0.009 | 4,126 | 3,533 | −0.27–1.46, 0.175 |
| Test group | Placebo group | |||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| Before application of electromagnetism | After application of electromagnetism | CI (95%), p* | Before application of electromagnetism | After application of electromagnetism | CI (95%), p* | |
| General energy (μA) | 19.62 | 13.50 | 3.10–9.15, < 0.001 | 18.83 | 15.04 | 0.76–6.82, 0.015 |
|
|
||||||
| Meridian energy (μA) | ||||||
| Lung | 22.73 | 15.33 | 1.74–13.05, 0.012 | 25.21 | 16.94 | 2.61–13.93, 0.005 |
|
|
||||||
| Pericardium | 19.58 | 10.15 | 4.46–14.41, < 0.001 | 19.48 | 13.30 | 1.21–11.61, 0.016 |
|
|
||||||
| Heart | 19.35 | 11.31 | 4.29–11.80, < 0.001 | 18.33 | 12.80 | 1.79–9.30, 0.005 |
|
|
||||||
| Small intestine | 21.83 | 14.43 | 2.10–12.69, 0.007 | 23.19 | 17.83 | 0.06–10.65, 0.047 |
|
|
||||||
| Triple heater | 29.73 | 24.95 | 0.33–9.21, 0.036 | 27.17 | 24.12 | −1.40–7.48, 0.174 |
|
|
||||||
| Large intestine | 30.06 | 20.75 | 3.71–14.92, 0.002 | 29.81 | 26.54 | −2.33–8.88, 0.246 |
|
|
||||||
| Spleen-pancreas | 17.71 | 13.16 | 0.91–8.17, 0.015 | 17.23 | 16.54 | −2.95–4.32, 0.705 |
|
|
||||||
| Liver | 18.21 | 13.08 | 0.90–9.35, 0.018 | 16.83 | 12.10 | 0.50–8.95, 0.029 |
|
|
||||||
| Kidney | 19.56 | 15.20 | −0.20–8.91, 0.061 | 18.29 | 14.44 | −0.70–8.41, 0.095 |
|
|
||||||
| Bladder | 11.43 | 8.10 | 0.56–6.11, 0.020 | 12.23 | 11.37 | −1.92–3.63, 0.538 |
|
|
||||||
| Gallbladder | 11.79 | 8.10 | 1.63–5.75, 0.001 | 10.41 | 8.18 | 0.17–4.29, 0.035 |
|
|
||||||
| Stomach | 18.83 | 13.91 | 0.96–8.87, 0.016 | 14.16 | 11.29 | −1.08–6.83, 0.150 |
- [1] Childress MA, Stuek SJ. Virginia commonwealth university Fairfax family practice, Fairfax, Virginia. Am Fam Physician 2020;102(3):150−156.PubMed
- [2] Global Burden of Disease. GBD 2017 disease and injury incidence and prevalence collaborators 2018.
- [3] Kay TM, Gross A, Goldsmith C, Santaguida PL, Hoving J, Bronfort G. Exercises for mechanical neck disorders. Cochrane Database Syst Rev 2005;(3):CD004250.. ArticlePubMed
- [4] White AP, Arnold PM, Norvell DC, Ecker E, Fehlings MG. Pharmacological management of chronic low back pain: synthesis of the evidence. Spine 2011;36(21 Suppl):S131−43.ArticlePubMed
- [5] Trombotto ML. Acupuncture in the treatment of chronic pain. São Paulo (Brazil), Brazilian School of Chinese Medicine, 2015, [in Portuguese].
- [6] Taffarel MO, Freitas PMC. Acupuncture and analgesia: clinical applications and main acupoints. Santa Maria Rural Sci 2009;39(9):2665−72. [in Portuguese].Article
- [7] Zhang B, Xie Y, Ni Z, Chen L. Effects and mechanisms of exogenous electromagnetic field on bone cells: a review. Bioelectromagnetics 2020;41(4):263−78.ArticlePubMedPDF
- [8] Bouché NF, McConway K. Melatonin levels and low-frequency magnetic fields in humans and rats: new insights from a bayesian logistic regression. Bioelectromagnetics 2019;40(8):539−52.ArticlePubMedPDF
- [9] Zhu S, He H, Zhang C, Wang H, Gao C, Yu X, et al. Effects of pulsed electromagnetic fields on postmenopausal osteoporosis. Bioelectromagnetics 2017;38(6):406−24.ArticlePubMedPDF
- [10] Karakaş M, Gök H. Effectiveness of pulsed electromagnetic field therapy on pain, functional status, and quality of life in patients with chronic non-specific neck pain: a prospective, randomized-controlled study. Turk J Phys Med Rehabil 2020;66(2):140−6.ArticlePubMedPMC
- [11] Sutbeyaz ST, Sezer N, Koseoglu F, Kibar S. Low-frequency pulsed electromagnetic field therapy in fibromyalgia. Clin J Pain 2009;25(8):722−8.ArticlePubMed
- [12] Vadalà M, Morales-Medina JC, Vallelunga A, Palmieri B, Laurino C, Iannitti T. Mechanisms and therapeutic effectiveness of pulsed electromagnetic field therapy in oncology. Cancer Med 2016;5(11):3128−39.ArticlePubMedPMCPDF
- [13] Gerken LRH, Gogos A, Starsich FHL, David H, Gerdes ME, Schiefer H, et al. Catalytic activity imperative for nanoparticle dose enhancement in photon and proton therapy. Nat Commun 2022;13(1):3248. ArticlePubMedPMCPDF
- [14] Pérez CN. Las biomediciones según el método Ryodoraku: el diagnostico de situación y su tratamiento. Madrid (Spain): Ediciones C.E.M.E.T.C.S.L; 2013. [in Spanish].
- [15] Nakatani Y, Yamashita K. Ryodoraku acupuncture: a guide for application of ryodoraku therapy electrical acupuncture, a new autonomic nerve regulating therapy. Tokyo. Ryodoraku Research Institute, 1977.
- [16] Wen TS. Classical Chinese acupuncture. 2001 São Paulo (Portugal): Editora Cultrix Ltda;2001. [in Portuguese].
- [17] Focks C, März U. Practical guide to acupuncture. Barueri (Brazil), Manole, 2008.
- [18] Yang X, He H, Ye W, Perry TA, He C. Effects of pulsed electromagnetic field therapy on pain, stiffness, physical function, and quality of life in patients with osteoarthritis: a systematic review and meta-analysis of randomized placebo-controlled trials. Phys Ther 2020;100(7):1118−31.ArticlePubMedPDF
- [19] Krueger-Beck E, Scheeren EM, Nogueira Neto GN, Nohama P. Electric and magnetic fields applied to peripheral nerve regeneration. Rev Neuroscience 2011;19(2):314−28.Article
- [20] Meyer PF, Cavalcanti APS, Silva EM, Silva RMV, Costa LS, Ronzio OA. Magnetotherapy: is it possible for this resource to be part of the Brazilian physiotherapist’s routine? Brazilian Health Sci Arch 2011;36(1):35−9.
- [21] Silvério-Lopes SM. Influence of the stimulatory frequency involved in the analgesic effects induced by electroacupuncture in tension neck pain. Braz J Phys Ther 2009;13(2):152−8. https://www.scielo.br/j/rbfis/a/HSbytpH3z3q9vzQSBBzSgQb/?format=pdf&lang=en.
- [22] Manafnezhad J, Salahzadeh Z, Salimi M, Ghaderi F, Ghojazadeh M. The effects of shock wave and dry needling on active trigger points of upper trapezius muscle in patients with non-specific neck pain: A randomized clinical trial. J Back Musculoskelet Rehabil 2019;32(5):811−8.ArticlePubMed
- [23] Zotelli VLR, Grillo CM, Gil MLB, Wada RS, Sato JE, Sousa MLR. Acupuncture effect on pain, mouth opening limitation and on the energy meridians in patients with temporomandibular dysfunction: a randomized controlled trial. J Acupunct Meridian Stud 2017;10(5):351−9.ArticlePubMed
- [24] Maciocia G. The fundamentals of Chinese medicine. São Paulo (Brazil), Roca, 2017.
- [25] Girach A, Aamir A, Zis P. The neurobiology under the placebo effect. Drugs Today (Barc) 2019;55(7):469−76.ArticlePubMed
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite